
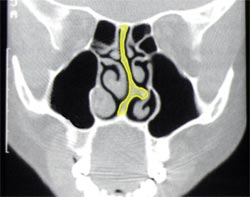
CT Scan of a deviated nasal septum. The septum (highlighted in yellow) shows a deviation towards the left that touches the lateral walls of the nose preventing
the passage of air.

The incision, within the nostril, through which the entire surgery for the correction of the nasal septum deviation is carried out.
At the end of the operation the incision will be closed
with 2-3 small absorbent sutures that will fall out without needing to be removed.
 Deviation of the nasal septum causing the nose as a whole to turn to the right. In these cases, it is impossible to obtain a straight nose without correcting both the cartilaginous and the osseous parts of the septum.
Deviation of the nasal septum causing the nose as a whole to turn to the right. In these cases, it is impossible to obtain a straight nose without correcting both the cartilaginous and the osseous parts of the septum.
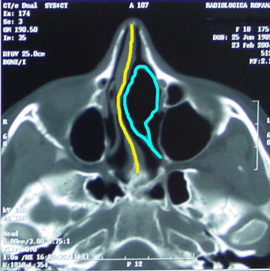 Deviation of the septum is sometimes caused by the presence of a “conca bullosa” (highlighted here in blue). In this congenital anomaly the middle turbinate contains a sort of air chamber that presses on the septum (in yellow) and causes it to deviate to one side. Its presence is revealed by nasal endoscopy and then confirmed by a CT scan. In these cases, it is impossible to obtain a straight septum without simultaneously carrying out rhinoplasty on the middle turbinate.
Deviation of the septum is sometimes caused by the presence of a “conca bullosa” (highlighted here in blue). In this congenital anomaly the middle turbinate contains a sort of air chamber that presses on the septum (in yellow) and causes it to deviate to one side. Its presence is revealed by nasal endoscopy and then confirmed by a CT scan. In these cases, it is impossible to obtain a straight septum without simultaneously carrying out rhinoplasty on the middle turbinate.
I breathe badly through my nose because I have a distorted nasal septum.
The nasal septum divides the nose into two nasal cavities. Through these external air reaches the pharynx and from here, moves through the larynx, the bronchial tubes and the lungs. The nasal cavities begin at the nostrils, which are the external openings, and finish at the choanae. The nasal septum is situated at the center and constitutes the dividing wall between the two nasal cavities. Sometimes the nasal septum is not situated centrally but tends toward one side: it follows that one of the nasal cavities will be of narrow dimensions and so it is more difficult for the air to pass through.
Other times the septum is situated in such a position that it creates a pronounced obstruction of both nasal cavities. This happens when a part of the nasal septum is positioned towards the right, and another towards the left. In addition to its position, the shape of the septum is also very important for the passage of air through the nose. Trauma to the nose, whether during infancy or adulthood, is often the origin of the deformity of the nasal septum. Often the cause of a nasal septum deviation is due to an incident that occurred while playing sport. In some cases the responsible trauma takes place at the moment of birth, with the passage of the head through the birth canal.
Another reason for deviation of the septum is a development anomaly and can also involve the palate and the teeth. In order to assess the presence and extent of a deviation of the nasal septum it is necessary to carry out an endoscopy of the nasal cavities as well as an external examination. Only this allows the examination of the septum's inner hidden areas, and will exclude the presence of other problems such as nasal polyps, or hypertrophy of the turbinates or adenoids.
There are other means to help establish whether it is worthwhile operating or not such as rhinomanometry, that allows you to measure air pressure and the rate of airflow in the nasal cavity.

Left: very visible deviation of the nasal septum because it involves the external caudal part of the septum. Right: result after the surgery: the nasal septum has been correctly repositioned in the center.
What can be done?
Through a surgical operation called septoplasty the shape and the position of the nasal septum can be corrected effectively eliminating those inner deformities of the nose that don't allow optimal passage of air. The septoplasty is usually carried out through a small internal incision in the nose, along the caudal margin of the septum. There are therefore no scars or stitches to remove. Through this small incision you reach the quadrangular cartilage, which constitutes the cartilaginous part of the septum, the vomer and the perpendicular plate of the etmoid, which constitute the bony parts.
The correction of the nasal septum is carried out by remodeling these structures with the minimal sacrifice of cartilage and bone: in this way after the operation there won't be disagreeable results visible on the externally like, for example, curvature of the nose or downward fall of the tip.
The surgery is preferably carried out in general anesthesia with the addition of a local anesthetic. This "mixed" method that unites the advantages of the general anesthesia to those of the local anesthesia allows complete elimination of post-operative pain. Except in unusual cases a septoplasty takes the surgeon between 2O and 30 minutes. The duration of recovery does not usually exceed 24 hours. Nevertheless today's modern anesthesiology techniques allow patients to shorten the period of their stay in hospital leaving the Clinic just hours after the operation, provided they are accompanied by someone and have permission from the surgical and anesthetic staff.
Today's modern techniques of internal nasal dissolvable sutures (that don't need to be removed) eliminate, in more than half of cases, the need to put packing in the nose. In the cases that require it (decided only during the surgery) pads will be left in the nose and will be removed after a period that varies from one to four days. The preferred nasal pads used are made from a special material (Lyofoam®) that has the characteristic of remaining very soft without adhering to the walls of the nose, thus they can be removed without any discomfort to the patient.